
As a doctor working in diagnostic imaging, I meet many people who book a scan because of breast pain—often with understandable worry about cancer. The reassuring reality is that breast pain on its own is usually not a sign of breast cancer, and in most cases it relates to hormonal change, benign breast tissue sensitivity, or chest-wall (muscle/rib) causes.
Key takeaways (the short version)
- Breast pain is common and often linked to periods, menopause transition, medication, or musculoskeletal strain.
- Pain alone is not routinely an indication for imaging in most pathways; imaging is used when there is separate clinical concern.
- When imaging is appropriate, targeted breast ultrasound is a key tool—especially for focal, persistent pain—sometimes alongside mammography depending on age and clinical context.
What breast pain is (mastalgia) and how I classify it clinically
Breast pain varies widely, so the pattern matters. In clinical practice, I think in four main categories:
1) Cyclical breast pain
This is pain linked to the menstrual cycle. A common pattern is discomfort that starts up to two weeks before a period and improves once the period begins or ends.
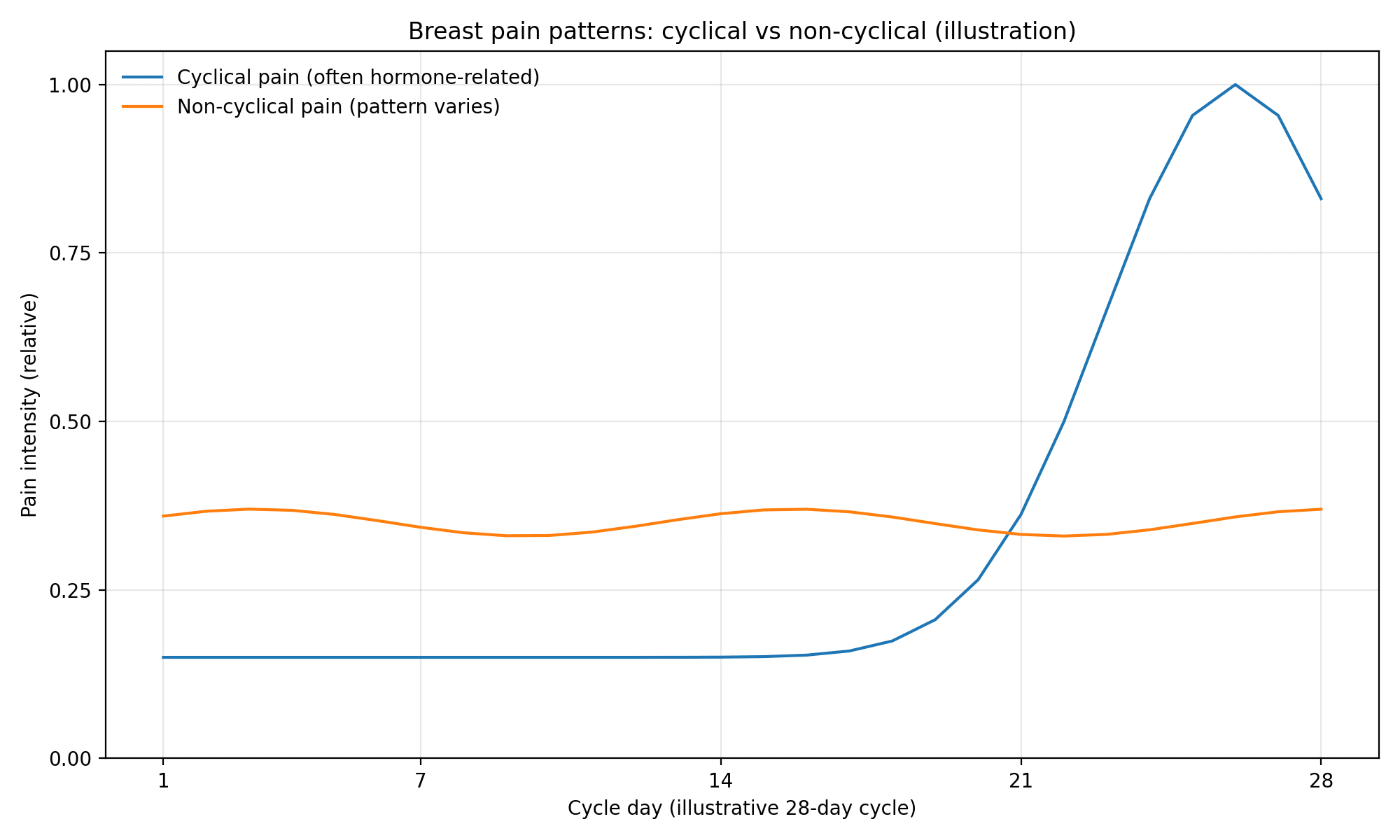
2) Non-cyclical breast pain
This is pain not clearly linked to the cycle. It may be intermittent or persistent.
3) Focal vs diffuse pain
Focal pain is localised—you can point to one spot. Diffuse pain feels more generalised across a larger area, often affecting both breasts.

4) True breast pain vs chest-wall pain
A common scenario is pain arising from muscles, ribs, or cartilage (for example, strain from exercise, posture, or costochondritis) that is felt as breast pain.
What breast pain usually means (common benign causes)
Most breast pain has a benign explanation. Common contributors include:
Hormonal sensitivity
Hormonal changes can make breast tissue feel heavy, tender, or sore—especially before periods, during perimenopause, or with contraception changes.
Menopause transition
Hormone fluctuations around menopause can cause intermittent tenderness, swelling sensations, or burning/aching discomfort.
Medication-related tenderness
Some people notice breast discomfort after starting or changing hormonal contraception, HRT, or certain antidepressants.
Inflammation or infection (mastitis/abscess)
This typically presents with redness, warmth, swelling, and systemic symptoms such as fever or feeling shivery—especially in breastfeeding, but not exclusively.
Benign breast cyst-related pain
Cysts are common and can be tender, particularly if they enlarge or fluctuate.
Musculoskeletal or referred pain
Neck/shoulder/back strain can refer pain to the breast region and may worsen with movement or pressure on the chest wall.
When to seek assessment (red flags I do not want you to ignore)
Even though breast pain is usually benign, pain plus other symptoms can require prompt assessment.
Seek urgent medical advice if you have breast pain with any of the following:
- A new or persistent breast lump
- Nipple discharge (especially blood-stained)
- Skin or nipple changes (dimpling, persistent rash, new inversion, peau d’orange)
- An axillary lump (swelling in the armpit)
- Redness, heat, swelling, or fever / feeling unwell
If your pain is persistent or worsening, or it interferes with sleep and daily life, it is also reasonable to seek assessment even without a classic red flag.
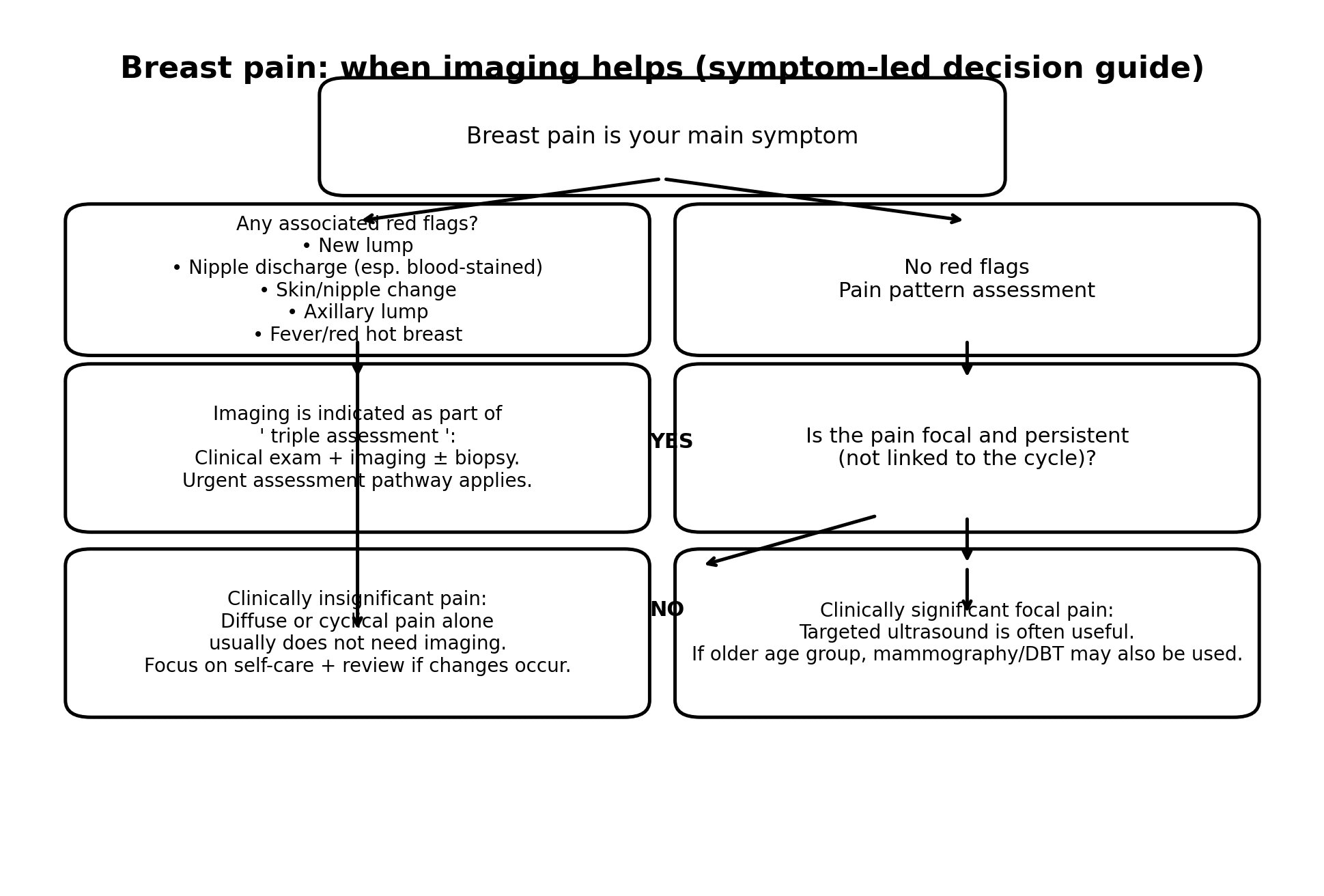
What happens in a symptom-led evaluation (how we decide if imaging is needed)
When your symptom is breast pain only, imaging is not always helpful. We use imaging when it is likely to change management—for example, when there is a lump, skin or nipple change, concerning discharge, or clinically significant focal symptoms with separate concern.
When imaging helps (practical decision rules)
Imaging is most helpful when:
- There is another concerning feature (lump, suspicious thickening, nipple discharge, skin/nipple change, or an axillary lump).
- Pain is clinically significant and focal (especially if persistent or non-cyclical), to look for treatable benign causes (for example, a cyst) and to provide appropriate reassurance.
Imaging is usually not helpful when:
- Pain is diffuse, bilateral, or clearly cyclical with no other concerning clinical features.
How breast ultrasound fits into symptom-led assessment
When imaging is appropriate, ultrasound is particularly useful because it is targeted (we scan the exact area you indicate), real-time, and it does not use ionising radiation.

Which test is used—ultrasound, mammography, or both?
This depends on age, symptoms, and clinical concern. In practice, focal, clinically significant pain may be assessed with ultrasound, and mammography may be added depending on age and overall presentation.
If your scan is normal but the pain continues
A normal scan is reassuring, but it does not always switch off symptoms—especially when pain is cyclical, hormonal, or chest-wall related.
- Ensure a well-fitted supportive bra.
- Consider simple pain relief if safe for you (discuss with your pharmacist/GP).
- Keep a brief symptom diary (location, cycle timing, triggers).
- Re-seek assessment if you develop new features (lump, discharge, skin/nipple change).
FAQs
Can breast pain be cancer?
Breast pain on its own is unlikely to be cancer. What matters is whether pain comes with other symptoms such as a lump, nipple discharge, or skin/nipple change, or whether it is focal and persistent with separate clinical concern.
When should I worry about breast pain?
If you have pain with a new lump, blood-stained nipple discharge, dimpling/skin change, nipple inversion/rash, redness/heat/swelling, or fever, seek urgent assessment.
If pain is linked to my period, do I need a scan?
Often, no. Cyclical pain is common and is usually managed conservatively unless there is a separate clinical concern.
Is ultrasound safe?
Yes. Ultrasound uses sound waves and does not use ionising radiation.
What if I’m over 40—does that automatically mean mammography?
Not automatically for pain alone. Imaging choice depends on the symptom profile and clinical concern. For focal, clinically significant pain, mammography may be considered alongside ultrasound depending on the overall picture.
Booking guidance
If you have breast pain plus any red-flag symptom, or you feel something new that concerns you, seek clinical assessment promptly. If your situation is appropriate for symptom-led imaging, you can book a private breast ultrasound at IUS London.
Next step: Book your appointment with IUS London


